Спонсорирано от:
Dreyfus Health Foundation
 DHF, 205 East 64 Street, Suite 404
DHF, 205 East 64 Street, Suite 404
New York, NY 10021
E-mail: Postmaster@thf.org
Fax
# 212-371-2776
Обръщение на главниЯ редактор
Уважаеми
колега,
В
ръцете си държите първия брой на бюлетина “Комуникации за по-добро здраве”,
съвместно издание на ВМИ - Плевен и Здравна фондация “Драйфус” - Ню Йорк. Както
личи от неговото заглавие, целите му са установяване на по-добри връзки между
медиците и всички, чиято основна цел е осигуряване на по-добро здраве за
населението. Вие ще имате достъп до пълните текстове на публикуваните резюмета
с посредничеството на библиотеката на ВМИ - Плевен.
Програмата
“Комуникации за по-добро здраве” е една от програмите на Здравна фондация
“Драйфус” - Ню Йорк..
Бюлетинът
ще излиза на четири месеца и ще съдържа следните материали:
1.Резюмета
от статии по здравни проблеми, по които се работи по проекти в рамките на програма
“Решаване на проблеми за по.добро здраве” в България.
2.
Материали по завършени и текущи проекти по програма”Решаване на проблеми за
по-добро здраве” в България.
3.
Текуща информация за минали и предстоящи мероприятия по здравни проблеми на
фондация “Драйфус” и на ВМИ - Плевен - семинари, срещи, дискусии, конференции,
научни сесии.
4.
Информация за програмите “Решаване на проблеми за по-добро здраве” и
“Комуникации за по-добро здраве” в други страни.
Новото
в настоящото издание е това, че той ще се стреми да осигури както информация по
здравни проблеми, така и обмен на информация между читателите си - той е достъпен за всички, които се интересуват
от материалите в него или желаят да публикуват свои материали.
Пожелавам
на всички вас добро здраве. Очакваме вашите мнения и препоръки.
Доц. д-р К. Игнатов, к.м.н.
Главен редактор
За Здравна фондациЯ “Драйфус”
Медицинска
фондация “Драйфус”е неправителствена организация, регистрирана преди 30 години от
Джак Драйфус, основател на фондовата корпорация “Драйфус”. Първо-началната цел
е да се спонсорират научни изследвания и да се разпространява информация за
фенитоин /дилантин/, лечението с който е помогнало на самия него. От 1970
година до днес са издадени три библиографии, които обобщават и анализират
медицинска литература по въпросите на фенитоина. Понастоящем библиотеката на
Фондацията разполага с над 16 000 заглавия на тази тема. През 1980 година Джак
Драйфус публикува “Едно забележително лекарство е подценено”, а през 1987
година се публикува второ преработено издание. През същата година се издава и
нова библиография - “Широкият спектър на клиничното приложение на фенитоина”, и
над 508 000 екземпляра от нея са разпространени безплатно сред лекарите в САЩ.
Тя е преведена на италиански, френски, руски, китайски, испански, немски и др.
През
1988 фондацията се преобразува в Здравна фондация и става част от института
“Рогозин”към Корнелския университетски медицинския колеж в Ню Йорк. Приоритети
за Корнелския медицински център са изследванията в областта на бъбречните
заболявания, атеросклерозата, раковите заболявания и диабета. Целта е
постиженията от изследванията да намерят бързо приложение в клиничната
практика. Сътрудничеството на центъра с фондация “Драйфус” разширява
възможностите на центъра да популяризира постиженията си.
В
продължение на 30 години Здравна фондация “Драйфус” спонсорира съвместни
клинични и здравни проучвания в Съединените щати, като събира, съхранява и
разпространява здравна информация, и като ръководи и присъства на национални и
международни срещи, семинари, конференции.
Здравна
фондация “Драйфус” е своебразен катализатор на мероприятия за подобряване на
здравето в много страни от света.
Програмата “Решаване на проблеми за по-добро здраве”
Стартира
през 1989 година с цел да се насърчат действията за подобряване на здравето.
Основен принцип в нея е да се използват наличните логистични, материални и
човешки ресурси, за да се разрешат проблемите на местна почва, да се поощрят
търсещите тези решения в техните индивидуални и колективни усилия за
разрешаването на конкретен проблем. За това спомага и начинът, по който се
организират семинарите - участниците не само биват обучавани как да търсят
решение на своите проблеми, но и да споделят своя опит и да се възползват от
опита на другите участници. За това определено допринася и участието на
фасилитатори от други страни, които споделят какви решения на подобни проблеми
са намерили те.
По
програмата “Решаване на проблеми за по-добро здраве” в момента се работи в
много страни - САЩ, Китай, Индия, Индонезия
/ на по няколко места/, в Бразилия, България, Камерун, Ел Салвадор,
Гана, Гвиана, Йордания, Нигерия, Полша, Словакия, Уганда, Полша, Замбия и др.
Contents
/ Съдържание
ABOUT DREYFUS HEALTH FOUNDATION
/ За здравна фондация “Драйфус”
MEDLINE INFORMATION /
ИНФОРМАЦИЯ ОТ MEDLINE
– Asthma / Астма
– Infant Feeding and Its Influence on Mother and Child Health /
Хранене на кърмачето и влияние на кърменето върху детското и майчиното здраве
– Drug Abuse / Наркомания
COMPLETED PSBH PROJECTS /
ЗАВЪРШЕНИ ПРОЕКТИ ПО ПРОГРАМА "РЕШАВАНЕ НА ПРОБЛЕМИ ЗА ПО-ДОБРО
ЗДРАВЕ"
–Adolescent Drug Abuse
Screening Study / Скринингово проучване на употребата и злоупотребата с
психоактивни вещества сред подрастващите
– Training Asthma Patients
/Обучение на болни с бронхиална астма с оглед ефективен контрол на заболяването
–AMI Prevention and Control / Профилактика и контрол на острия миокарден
инфаркт
PROJECTS IN ACTION / СЪОБЩЕНИЯ
ПО ДЕЙСТВАЩИ ПРОЕКТИ
– Breast Feeding Promotion /
Създаване на колективи “приятели на кърмачето”
– Respiratory Infections
Prevention in Asthma Patients by Respivax and Vaxigrip/Influvac / Профилактика
на респираторните инфекции при болни с бронхиална астма с respivax и противогрипна
ваксина
– Prevention of Accidental Poisoning of Children / Да предпазим децата
от отравяне
– OTHER PROJECTS IN ACTION /
ИНФОРМАЦИЯ ЗА ПРОЕКТИ В ХОД
REQUEST FORM AND QUESTIONNAIRE
/ ФОРМУЛЯР ЗА ПОРЪЧВАНЕ НА СТАТИИ И ВЪПРОСНИК
ASTHMA / АСТМА
The deeper we go into the
human body using modern technologies the more we appreciate the need to talk to
the patient. Bronchial asthma is a chronic disease. There have recently been
studies which gave therapeutic, psychological and economic facts suggesting
that patient education is important. Here below one can find some titles and
abstracts from articles on that issue.
Колкото повече научаваме за
човешкия организъм, ползвайки се от съвременните технологии, толкова повече
осъзнаваме необходимостта да общуваме с пациента. Бронхиалната астма е хронично
заболяване. Напоследък се провеждат редица проучвания, които разглеждат астмата
в клиничен, психологически и икономически аспект, от които става ясно, че
обучението на пациента с астма не е без значение. Тук публикуваме някои
заглавия и резюмета на статии по проблема.
д-р Явор Иванов
TI: Randomised trial of an
asthma self-management programme for adults.
AU: Allen RM.
Jones MP. Oldenburg B.
AD: Department of Health Promotion and Patient
Education, Royal North Shore Hospital, Australia.
SO: Thorax.
50(7):731-8, 1995 Jul.
BACKGROUND: A hospital based, community
service asthma education programme for adults to improve asthma knowledge,
promote compliance with medication, and reduce morbidity was evaluated. METHODS:
The programme was evaluated using a randomised experimental and control group
design with repeated measurements over 12 months. A volunteer community sample
of 192 respondents was recruited of whom 116 satisfied the inclusion criteria.
At the 12 month follow up some data were obtained for all subjects.
Intervention subjects attended four 2.5 hour education sessions at weekly
intervals. An asthma knowledge questionnairewas administered and compliance was
assessed from diary records. Morbidity was assessed retrospectively by
questionnaire, prospectively by diary, and objectively by spirometry and serial
peak expiratory flow rate monitoring. The adequacy of medical treatment was
also assessed. Data were collected at baseline, immediately after the intervention,
and at three, six, nine, and 12 months after intervention. RESULTS-
Improvements occurred in knowledge and compliance in the intervention group but
the impact on morbidity was modest; this was due, at least in part, to the
inadequacy of medical treatment. CONCLUSIONS- Treatment of asthma should be
reviewed and optimised in conjunction with self-management programmes in order
to improve health outcomes.
TI: Evaluation of an asthma
self-management education program.
AU: Boulet LP.
Boutin H. Cote J. Leblanc P.
Laviolette M.
AD: Le Centre de Pneumologie de l’Hopital
Laval, Universite Laval Sainte-Foy, Quebec, Canada.
SO: J Asthma.
32(3):199-206, 1995.
The goal of this study was to evaluate a
self-management education program for asthmatics. This was a case-controlled
retrospective study with a “1 year before and 1 year after” assessment of the
proposed education program. It was carried out in the Quebec City metropolitan
area, tertiary-center setting. The intervention group included 42 patients, 14
men and 28 women, aged 15-71 years. A control group of 42 patients was matched
for age, sex, and medication needs. Neither of the 2 groups had previously
received structured asthma education. The intervention group received 3
training sessions on asthma and its treatment, the use of action plans and
self-measurement of peak expiratory flow, and was offered individual teaching
by a specialized educator or telephone consultation.
Evaluation of asthma knowledge was made before and after
the teaching sessions and 1 year later. The control group received their usual
care. The primary clinical outcome measures included frequency of
asthma-related emergency-room (ER) visits, hospitalizations, absenteeism from
work, and quality of life, measured 1 year prior to initiation of the
educational program and for 1 year after, using questionnaires, chart reviews,
and interviews. The control group was evaluated only during the last year of
the study. Knowledge of asthma and its management was significantly improved immediately
after the program and 1 year later (both p < 0.001).
TI: Effect of patient education on asthma
management.
AU: Brewin AM.,
Hughes JA.
SO: Br J
Nurs. 4(2):81-2, 99-101, 1995 Jan
28-Feb 8.
Patients need to understand their asthma
to be able to react appropriately. At least 30 minutes is needed by a trained
asthma professional to teach asthma self-management effectively. Many patients
accept symptoms and attacks unnecessarily through insufficient knowledge of
their condition and treatment. In this small study, those who were educated by
a trained asthma nurse had a significantly higher knowledge of their condition
and management. Most of those who were educated by a trained asthma nurse had
symptoms less frequently. Those who were educated by a trained asthma nurse had
no time off work whereas 49% of the control group had time off work.
TI: Do clinical guidelines introduced with
practice based education improve care of asthmatic and diabetic patients? A
randomised controlled trial in general practices in Еast London.
AU: Feder G.
Griffiths C. Highton C. Eldridge S.
Spence M. Southgate L.
AD: Department of General Practice and Primary
Care, St. Bartholomew’s and Royal London
Hospital Medical College, UK.
SO: BMJ.
311(7018):1473-8, 1995 Dec 2.
OBJECTIVE: To determine whether locally
developed guidelines on asthma and diabetes disseminated through practice based
education improve quality of care in non-training, inner city general
practices. DESIGN: Randomised controlled trial with each practice receiving one
set of guidelines but providing data on the management of both conditions.
SUBJECTS: 24 inner city, non-training general practices. SETTING: East London.
MAIN OUTCOME MEASURES: Recording of key variables in patient records (asthma:
peak flow rate, review of inhaler technique, review of asthma symptoms,
prophylaxis, occupation, and smoking habit; diabetes: blood glucose
concentration, glycaemic control, funduscopy, feet examination, weight, and
smoking habit); size of practice disease registers; prescribing in asthma; and
use of structured consultation “prompts.” RESULTS: In practices receiving
diabetes guidelines, significant improvements in recording were seen for all
seven diabetes variables. Both groups of practices showed improved recording of
review of inhaler technique, smoking habit, and review of asthma symptoms. In
practices receiving asthma guidelines, further improvement was seen only in
recording of review of inhaler technique and quality of prescribing in asthma.
Sizes of disease registers were unchanged. The use of structured prompts was
associated with improved recording of four of seven variables on diabetes and
all six variables on asthma. CONCLUSIONS: Local guidelines disseminated via
practice based education improve the management of diabetes and possibly of
asthma in inner city, non-training practices. The use of simple prompts may
enhance this improvement.
TI: Using quality-control analysis of peak
expiratory flow recordings to guide therapy for asthma
AU: Gibson PG.
Wlodarczyk J. Hensley MJ. Murree-Allen K. Olson LG. Saltos N.
AD: Respiratory Medicine Unit, John Hunter
Hospital, New South Wales, Australia.
SO: Ann Intern Med. 123(7):488-92, 1995 Oct 1.
OBJECTIVE: To compare the action points
in published asthma management plans with those derived from quality-control
analysis of peak expiratory flow recordings. DESIGN: Longitudinal observational
study. SETTING: An ambulatory asthma education and management program in a
tertiary care hospital. PATIENTS: 35 adults with asthma and exacerbation of
asthma. MEASUREMENTS: Peak expiratory flow diaries and symptom recordings.
RESULTS: Asthma action points from published asthma management guidelines had
poor operating characteristics. The success rate was 35% when the action point
was a peak expiratory flow rate less than 60% of the patient’s best peak flow.
The success rate improved to 88% when the action point was a peak expiratory
flow rate less than 80% of the patient’s best peak flow. Published action
points had a high failure rate. Peak flow decreased to below the published
action points during a stable period of asthma in 7% to 51% of patients
studied. Action points defined using quality-control analysis did significantly
better. A peak flow value less than 3 standard deviations below the patient’s
mean peak flow detected 84% of exacerbations and had a low failure rate (19%).
Other quality-control tests had sensitivities of 91% and 71%. Quality-control
action points could detect exacerbations up to 4.5 days earlier than
conventional methods. CONCLUSIONS: Individualized action points can be derived
for patients with asthma by applying quality-control analysis to peak flow
recordings. These action points are more sensitive in detecting exacerbations
of asthma and have fewer false-positive results. Action plans developed in this
manner should be more useful for the early detection of deteriorating asthma.
TI: Self-management, autonomy, and quality
of life in asthma. Population Medicine Group 91C.
AU: Gibson
PG. Talbot PI. Toneguzzi RC.
AD: Asthma
Management Service, John Hunter Hospital, Newcastle, New South Wales.
SO: Chest. 107(4):1003-8, 1995 Apr.
STUDY OBJECTIVE: Asthma management guidelines
emphasize increased autonomy for asthmatics through patient education and
patient-initiated action plans. The aim of this study was to examine autonomy,
as reflected in the preferences of asthmatic subjects for decision making and
their preferences for information seeking. The results were related to quality
of life in asthma. SUBJECTS: One hundred
twenty-three adults with asthma. DESIGN: Questionnaire-based
cross-sectional analytic survey. SETTING: Eighty-five subjects were recruited
from community pharmacies at the point of sale of albuterol inhalers for asthma
and compared with 38 subjects recently hospitalized for acute severe asthma.
MEASUREMENTS: Asthma-related quality of life, autonomy preferences
questionnaire. RESULTS: The subjects in both groups had a mild-to-moderate
quality of life impairment in all domains that was greater in the
posthospitalization group (p < 0.05). Both groups expressed strong
preferences for information concerning their condition (92se 0.8, 91se 1.1, out
of a possible 100). Subjects did not prefer to MAKE DECISIONS ALONE ABOUT THE
MANAGEMENT OF ASTHMA EXACERBATIONS{INCLUDE IT AS A QUESTION} (51.0se 1.2, 52.5
se2.0, out of a possible 100). As the
severity of the asthma exacerbation increased, the desire to make decisions
decreased (p < 0.05). Older subjects expressed less desire for decision
making than younger subjects. Self-management autonomy was not correlated with
quality of life in asthma. CONCLUSIONS: We conclude that while asthmatics have
strong desires to be informed about their illness, they do not wish to be the
prime decision makers during an exacerbation. These findings have implications
for the success of self-management programs and action plans.
TI: Asthma self-management education program
by home monitoring of peak expiratory flow.
AU: Ignacio-Garcia
JM. Gonzalez-Santos P.
AD: Unit of
Pneumonology, General Hospital of Serrania, Ronda, Spain.
SO: Am J Respir
Crit Care Med. 151(2 Pt 1):353-9, 1995
Feb.
A prospective controlled trial of home
monitoring of peak expiratory flow rate (PEFR) was conducted to determine the
usefulness of an objective measure of lung function in association with an
education program and a medication self-management plan in reducing morbidity
in adult patients with asthma. Thirty-five patients managed themselves, using
peak flow readings as the basis for the therapeutic plan coupled with
educational intervention, whereas 35 control patients used symptoms and
spirometric data for following physicians’ treatment plans. After a 6-mo study
period, patients in the experimental group showed statistically significant
improvements in morbidity parameters (days lost from work, acute asthma
attacks, days on antibiotic therapy, physician consultations, and emergency room
admissions for asthma), increases in FVC, FEV1, and FEV1/FVC, mean PEFR and
mean morning PEFR, decrease in percentage of the mean PEFR amplitude, and a
reduction in the use of inhaled beta-agonists, oral theophylline, and oral
prednisone. Although improvements in some of these parameters were also found
in the control group, they did not reach the levels of significance obtained in
the experimental group. The personal use of an objective measure of lung
function in association with a medication self-management plan leads to
improvement in the patient’s condition.
TI: How to implement an asthma education
program. [Review]
AU: Kohler CL.
Davies SL. Bailey WC.
AD: Department of Health Behavior, University
of Alabama at Birmingham School of Public Health, USA.
SO: Clin Chest Med. 16(4):557-65, 1995 Dec.
Given that poor asthma management leads
to such devastating rates of morbidity and mortality in this country, efforts
must be made to increase the knowledge, skills, and behaviors of persons with
asthma. The suggestions and recommendations provided here represent a blend of
academic opinion and practical advice on methods to implement an asthma
education program. In developing an asthma education program, consideration
must be given to what content should be included, how and by whom that content
should be taught, and when education should take place. The identification of a
key clinical staff member to take the lead in translating these and other
asthma education guidelines will be a critical next step for clinicians
committed to developing an effective asthma education program. [References: 18]
TI: Randomised comparison of guided self
management and traditional treatment of asthma over one year.
AU: Lahdensuo A. Haahtela T. Herrala
J. Kava T. Kiviranta K. Kuusisto
P.Peramaki E. Poussa T. Saarelainen S. Svahn T.
AD: Department of Pulmonary Diseases, Tampere
University Hospital, Pikonlinna, Finland.
SO: BMJ.
312(7033):748-52, 1996 Mar 23.
OBJECTIVE: To compare the efficacy of self
management of asthma with traditional treatment. DESIGN: 12 month prospective
randomised trial. SETTING: Outpatient clinics in Finland. SUBJECTS: 115
patients with mild to moderately severe asthma. INTERVENTIONS: Patient
education and adjustment of anti-inflammatory therapy guided by peak flow
measurements. MAIN OUTCOME MEASURES: Unscheduled admissions to hospital and
outpatient visits, days off work, courses of antibiotics and prednisolone, lung
function, and quality of life. RESULTS: The mean number of unscheduled visits
to ambulatory care facilities (0.5 v 1.0), days off work (2.8 v 4.8), and
courses of antibiotics (0.4 v 0.9) and prednisolone (0.4 v 1.0) per patient
were lower and the quality of life score (16.6 v 8.4 at 12 months) higher in
the self management group than in the traditionally treated group. In both
groups admissions for asthma were rare. CONCLUSIONS: Self management reduces
incidents caused by asthma and improves quality of life.
TI: Patients’ interest in educational
programmes on asthma.
AU: Moscato
G. Niniano R. Corsico A. Cretti L. Colli
MC. Perfetti L. Bianchi P.
AD: School of
Allergology and Clinical Immunology, University of Pavia, Italy.
SO: Monaldi Arch
Chest Dis. 50(4):319-22, 1995 Aug.
The compliance of patients in
educational programmes on asthma is sometimes lacking and this may be due in
part to patients’ scarce interest or refusal to expand their knowledge of the
disease. In the present study, we aimed to evaluate the interest of a group of
asthmatic patients in education on asthma and to point out the asthma-related
topics considered particularly worth discussing. The study was conducted before
starting the educational programme. Sixty adult patients with mild-to-moderate
asthma were asked to complete a questionnaire, including a group of 14
questions aimed at evaluating the level of patients’ interest in various
asthma-related topics, one question regarding patients’ willingness to attend a
small-group educational course on asthma, and a further question asking
patients to suggest topics of particular interest for discussion. For each of
the first 14 questions, patients indicated their level of interest according to
a score ranging 1-3. The sum of the scores obtained for each topic (partial
score) and the sum of partial scores (total score) were calculated and
classified into three classes of interest (I: low, II: medium; III: high), and
the distribution of patients into the three classes was analysed (chi-squared
test).
TI: Asthma: lessons from patient education
AU: Partridge
MR.
SO: Patient Educ
Couns. 26(1-3):81-6, 1995 Sep.
Asthma is a common condition. Recent
understanding of the disease has meant that the inflammatory process in the
airways is likely to be treated by the regular use of preventative therapy even
when the patient is well. The evidence suggests that such treatment is often
not taken. Audit suggests that poor communication and lack ofinformation
remains a common problem. There is increasing use of a TEAM APPROACH to the
management of asthma, often necessitated by the sheer numbers of patients
requiring regular review. Such an approach combined with the giving of control
of their own condition to the patients, has now been shown to improve outcomes.
TI: Delivering optimal care to the person with
asthma: what are the key components and what do we mean by patient education?
[Review]
AU: Partridge MR.
AD: Whipps Cross Hospital, London, UK.
SO: Eur Respir J.
8(2):298-305, 1995 Feb.
The new understanding of the pathogenesis
of asthma has led to an increasing perception of the disease as a chronic
condition, rather than one consisting of acute exacerbations. Health
professionals need to help patients to accept this new understanding, and this
involves a consideration of how best to deliver care and how best to enhance
compliance. GOOD COMMUNICATION is essential, and STRUCTURED PATIENT EDUCATION
has now been shown to be cost effective. All health professionals need to think
how education may best be incorporated into their care. Such care will involve
the development of a partnership between health professional and the patient
and their loved ones, and the acquisition by patients of skills in
self-management. Several unknowns remain regarding who benefits more from group
education as opposed to individual education, and some details of guided
self-management. However, in the face of clear evidence of the benefits of
patient education, these areas for further study should not delay the adoption
of a strong commitment to education by all of those who care for those with
asthma. [References: 72]
TI: Pharmacist-managed, physician-directed
asthma management program reduces emergency department visits.
AU: Pauley TR. Magee MJ.
Cury JD.
AD: Department of
Pharmacy, University of Florida Health Scence Cener/Jacksonville Unversity
Medical Center.
SO: Ann
Pharmacother. 29(1):5-9, 1995 Jan.
OBJECTIVE: To determine whether the
number of emergency department (ED) visits for acute asthma exacerbations could
be decreased by providing patients with a comprehensive program of asthma
management delivered by a pharmacist and a physician. DESIGN: Patients were
selected from the ED and asked to attend a special asthma clinic that provided
education about asthma and proper use of asthma medications, regular telephone
contact between the pharmacist and patient, and an open-door clinic policy.
SETTING: A university-affiliated urban teaching hospital. PARTICIPANTS: The
study population consisted of 25 asthmatic patients who were at least 18 years
of age and who were seen in the ED a minimum of 3 times in a 12-month period.
MAIN OUTCOME MEASURES: The number of visits to the ED for acute exacerbations
of asthma was measured. Patients served as their own controls. The number of ED
visits for asthma during the 6-month study period was compared with two 6-month
periods prior to the study period for each patient. RESULTS: The total number
of ED visits for the 25 enrolled patients six months prior to their enrollment
into the study was 92; the number of ED visits during the same months of the
study in the prior year was 47. During the study period, there were only 6 ED
visits for asthma exacerbations. CONCLUSIONS: The comprehensive asthma
management program reduced the number of ED visits for acute exacerbations of
asthma.
TI: Physicians’ prevention-related
practice behaviors in treating adult patients with asthma: results of a
national survey.
AU: Wolle JM. Cwi J.
AD: National
Institutes of Health, NHLBI/DLD, Bethesda, MD 20817, USA.
SO: J Asthma. 32(2):131-40, 1995.
To improve the health outcome of adults
with asthma, it is important to understand the current practice behaviors of
physicians related to the prevention and treatment of asthma. A national survey
was conducted to ascertain the practice behaviors of physicians in five
specialty areas: internal medicine, pulmonary, allergy/immunology, occupational
health, and family health. Similarities and differences in practice among the
specialty areas are indicated. The data provide a basis for recommendations to
improve the management of asthma by standardizing history taking, increasing
the use of pulmonary function testing, and using effective counseling and
patient education strategies.
INFANT FEEDING AND ITS INFLUENCE ON MOTHER AND CHILD HEALTH / ХРАНЕНЕ НА КЪРМАЧЕТО И ВЛИЯНИЕ НА
КЪРМЕНЕТО ВЪРХУ ДЕТСКОТО И МАЙЧИНОТО ЗДРАВЕ
In the first issue of the
digest,16 abstracts are included,concerning:
·
Infant’s feeding policy
·
Breast feeding and infant’s morbidity and mortality
·
Influence of lactation and nursing on women
These abstracts are only a
very few from the latest publications devoted to breast-feeding, and illustrate
the actuality of the problem.
В първия брой на бюлетина
са включени 16 резюмета по въпросите на
·
Храненето на детето до една година
·
Кърмене и детска заболеваемост и смъртност
·
Влияние на лактацията и кърменето върху майчиното здраве
проф. д-р Никола Мумджиев
TI: Breast-feeding in London, 1905-19
AU: Fildes V.
SO: Journal of Biosocial Science 24:53-70,
1992.
Medical Officer of Health reports for
London boroughs, 1900-19, are analysed to determine the incidence of neonatal
breast- feeding, duration of lactation, reasons for early supplementation and
premature weaning, and their relationship with infant mortality. In a sample of
222,989 infants, breast-feeding rates were very high. Over 90% were breast-fed
in the first month, almost 80% at 3 months, and over 70% at 6 months. The
poorest boroughs had the highest rates of neonatal breast-feeding, but also a
higher incidence of early supplementation and premature weaning. There was a
significant positive correlation between breast-feeding and infant mortality
due to poor maternal diet and health, poor nutritional quality of supplementary
and substitute foods, and the use of anunhygienic feeding bottle. Energetic
campaigns to counteract these problems probably contributed to the fall of
infant mortality in this period.
TI: The effect of postpartum lactation
counseling on the duration of breast-feeding in low-income women
AU: Grossman LK,
Harter C, Sachs L, Kay A
SO: American
Journal of Diseases of Children 144:471-474, 1990.
We investigated the effectiveness of a
program of intensive postpartum support for low-income, breast-feeding women
and identified potential predictors of prolonged breast-feeding in this
population. Ninety-seven low-income women were randomized to receive intensive
postpartum education and support for breast-feeding or to receive only the
routine assistance provided by the obstetrical nurses. Both groups were
telephoned 6 weeks post partum to determine the method of infant feeding then,
and those still breast-feeding were contacted monthly until complete weaning
had occurred. No significant difference in breast-feeding duration between the
two groups was noted. There was no association between duration of nursing and
race, marital status, or the need to return to work or school. Earlier age at
introduction of upplement, younger maternal age, and participation in prenatal
classes predicted breast-feeding duration by logistic regression.
TI: Infant feeding policies in maternity
wards and their effect on breast-feeding success: an analytical overview
AU: Perez-Escamilla
R, Pollitt E, Lonnerdal B, Dewey KG
SO: American Journal
of Public Health 84:89-97, 1994.
OBJECTIVES: The purpose of this review
is to examine the plausibility of a causal relationship between maternity ward
practices and lactation success. METHODS: Studies were located with MEDLINE,
from our personal files, and by contacting researchers working in this field.
Of the 65 studies originally reviewed, 18 met our inclusion criteria (i. e.,
hospital-based intervention, experimental design with randomization procedures,
or quasi-experimental design with adequate documentation). RESULTS:
Meta-analysis indicated that commercial discharge packs had an adverse effect
on lactation performance. The impact of early mother-infant contact on
lactation success was unclear. Rooming-in and breast-feeding guidance in a rooming-in
context had a beneficial impact on breast-feeding among primiparae.
Breast-feeding on demand was positively associated with lactation success.
In-hospital formula supplementation of 48 mL per day was not associated with
poor breast-feeding performance. CONCLUSIONS: Hospital-based breast-feeding
interventions can have a beneficial effect on lactation success, particularly
among primiparous women.
TI: Effects of age of introduction of complementary
foods on infant breast milk intake, total energy intake, and growth: a
randomised intervention study in Honduras
AU: Cohen RJ, Brown
KH, Canahuati J, Rivera LL, Dewey KG
SO: Lancet
344:288-293, 1994.
In developing countries, the age at
which breastfed infants are first given complementary foods is of public health
importance because of the risk of diarrhoeal disease from contaminated weaning
foods, and the potential risk of growth faltering if foods are inappropriately
delayed. To evaluate whether there are any advantage of complementary feeding
prior to 6 months, low- income primiparous mothers who had exclusively
breastfed for 4 months were randomly assigned to one of 3 groups: continued
exclusive breastfeeding to 6 months (EBF) (n = 50); introduction of
complementary foods at 4 months with ad libitum nursing from 4- 6 months (SF)
(n = 47); and introduction of complementary foods at 4 months, with maintenance
of baseline nursing frequency from 4-6 months (SF-M) (n = 44). Baby foods in
jars were provided to the SF and SF-M groups from 4 to 6 months. Subjects were
visited weekly and provided with lactation guidance; at 4, 5, and 6 months
measurements were made of infant intake and breast milk composition. At 4
months, breast milk intake averaged 797 (139) g per day (no difference among
groups). Between 4 and 6 months, breast milk intake was unchanged in EBF
infants (+6) but decreased in the SF (-103), and SF-M (-62) groups (p <
0.001). Change in total energy intake (including solid foods) and infant weight
and length gain did not differ significantly between groups. Weight and length
gain from 4-6 months were comparable to those of breastfed infants in an
affluent USA population. The results indicate that breastfed infants
self-regulate their total energy intake when other foods are introduced. As a
result, there is no advantage in introducing complementary foods before 6
months in this population, whereas there may be disadvantages if there is
increased exposure to contaminated weaning foods.
TI: Health service support of breast feeding: are we
practising what we preach?
AU: Beeken S, Waterston T
SO: British Medical Journal 305:285-287,
1992.
OBJECTIVE: To ascertain the attitudes of
health professionals and breast feeding mothers to breast feeding and their
views on current practice. DESIGN: Questionnaire to all midwives and health
visitors and to breast feeding mothers in Newcastle upon Tyne. SETTING:
Maternity units and community in Newcastle upon Tyne. SUBJECTS: 127 hospital
midwives, 23 community midwives, 63 health visitors, and 50 first time breast
feeding mothers. RESULTS: Optimum practice guidelines were not followed. 30
(60%) mothers said they were separated from their babies on the first night
after birth. 82 (42%) professionals said that breast fed babies were frequently
given water to drink. 28 (56%) babies in the mothers survey had received food
or water other than breast milk; 19 of these had been given water.
Professionals expressed mainly positive attitudes towards breast feeding in
general but less positive attitudes to specific issues such as the beneficial
effects on child health and the value of voluntary organisations in
breastfeeding promotion and management. CONCLUSIONS: Although many health
workers are in favour of breast feeding there is conflict among the professions
working most closely with breast feeding mothers. Good breast feeding support
requires closer attention to monitoring hospital practices and continued
training on good lactation management.
TI: Breast-feeding of very low birth weight infants.
AU: Bier JB, Ferguson A, Anderson L, Solomon
E, Voltas C, Oh W, Vohr BR
SO: Journal of Pediatrics 123:773-778, 1993.
Twenty very low birth weight infants
(birth weight < 1500 gm) were assessed to compare the clinical effects of
breast and bottle feedings. The infants started breast-feeding during the same
week that they started bottle feedings. Five breast-feedings and five bottle
feedings for each infant were observed. Axillary temperature and weight before
and after feedings were measured, and oxygen saturation, respiratory rate, and
heart rate were monitored and recorded every 2 minutes during the feeding
periods. The results showed no difference in oxygen saturation during
breast-feeding (p = 0.056) but a lower incidence of oxygen desaturation (<
90%) (21% vs 38% in breast-feeding vs bottle feeding, respectively; p
<0.025). Infants with bronchopulmonary dysplasia had higher oxygen
saturation during breast-feeding than during bottle feeding (p < 0.025), but
weight gain during breast- feeding sessions was less (median, no gain vs 31 gm,
p < 0.001). We conclude that (1) very low birth weight infants can tolerate
both breast and bottle feedings at the same postnatal age; (2) very low birth
weight infants are less likely to have oxygen desaturation to less than 90%
during breast-feeding; and (3) weight gain is less during breast-feeding,
probably because of lower intake, and may require more lactation counseling or
supplementation of the feedings.
TI: Effects of feeding and social factors on diarrhoea and
vomiting in infants.
AU: Eaton-Evans J, Dugdale AE
SO: Archives of Disease in Childhood
62:445-448, 1987.
In a prospective study of infants and
their feeding in south east Queensland, Australia, the incidences of reported
diarrhoea and/or vomiting in breast, bottle, and mixed (breast and bottle) fed
infants were compared from birth to 1 year. Up to 6 months infants who were
given breast feeds, with or without other milks, had less diarrhoea and/or
vomiting than those given bottle feeds only. Breast feeding seemed to protect
the infant against possible introduced infections even when other milks were
given along with the breast milk. After 6 months breast feeding did not reduce
the incidence of gastrointestinal infection. In both upper and lower social
class families infants given solids before 3 months had less diarrhoea and/or
vomiting than those given solids later. Bottle fed infants aged 3-6 months in
upper social class families had fewer gastrointestinal problems than those of
lower social class families. This study suggests that up to the age of 6
months, in this population, breast feeding protects the infant against
diarrhoea and/or vomiting, but other milks and solids can safely be given to
supplement the breast milk. Breast feeding conferred no significant protection
after 6 months.
TI: Human milk in the management of protracted diarrhoea of
infancy
AU: Macfarlane PI, Miller V
SO: Archives of Disease in Childhood 59:260-265,
1984.
Eleven of 13 children with the
protracted diarrhoea syndrome of infancy were successfully treated with human
milk. All the infants, who were severely malnourished, had deteriorated while
fed on a wide range of highly modified formulas. Seven infants responded
promptly with cessation of weight loss and diarrhoea; in four others, human
milk was used to re-establish oral nutrition after a period of intravenous
nutrition when all other measures had failed. Two children did not respond to
human milk. Despite its high lactose content, human milk has nutritional and
immunological properties that may reverse many of the factors thought to cause
the protracted diarrhoea syndrome, and we conclude that it has an important
role in management of this syndrome and may obviate the need for intravenous
nutrition as a life saving measure.
TI: Protection of breast-fed infants against Campylobacter
diarrhea by antibodies in human milk
AU: Ruiz-Palacios GM, Calva JJ, Pickering
LK, Lopez-Vidal Y, Volkow P, Pezzarossi H, West MS
SO: Journal of Pediatrics 116:707-713, 1990.
To investigate the role of
breast-feeding in preventing diarrhea caused by Campylobacter jejuni, we
followed 98 Mexican children prospectively for 2 years beginning at their
birth. Attack rates of diarrhea in children less than 6 months of age who were
not fed human milk were 2.3 times greater than those in children of the same
age who were fed human milk. Breast-fed children remained free of diarrhea for
a longer time than non-breast-fed children (p less than 0.0005). The diarrhea
attack rate caused by C. jejuni for non-breast-fed infants was significantly
greater (p less than 0.005) than that in the breast-fed group. Secretory IgA
milk antibody titers against glycine acid-extractable antigen of C. jejuni were
high in colostrum, decreased during the first month of breast-feeding, and
generally persisted throughout lactation. Human milk consumed by children in
whom Campylobacter diarrhea developed did not contain secretory IgA antibodies
to the glycine acid-extractable common antigen of Campylobacter. This study
shows an association between Campylobacter antibodies in human milk and
prevention of diarrhea caused by Campylobacter.
TI: Infant feeding and allergy
AU: Miskelly FG, Burr ML, Vaughan-Williams
E, Fehily AM, Butland BK, Merrett TG
SO: Archives of Disease in Childhood
63:388-393, 1988.
The effect of withholding cows’ milk was
examined in 487 infants at high risk of allergic disease. Before birth they
were randomly allocated either to a control group, most of whom received cows’
milk preparations, or to an intervention group, who were offered a soya based
substitute. Eczema and wheezing occurred to a similar extent in the two groups
during the first year of life, although napkin rash, diarrhoea, and oral thrush
were commoner in the intervention group, especially during the first three
months. Breast feeding for any length of time was associated with a reduced
incidence of wheezing and diarrhoea.
TI: Infant feeding and allergy: 12-month
prospective study of 500 babies born into allergic families. [Review]
AU: Merrett TG,
Burr ML, Butland BK, Merrett J, Miskelly FG, Vaughan-Williams E
SO: Annals of
Allergy 61:13-20, 1988
This investigation studied 487 babies for
symptoms of allergic disease during their first year of life. Because of their
positive family histories all the babies are at high risk of becoming allergic.
The babies were randomly divided such that cows’ milk was deliberately withheld
from one group; infants in this group were fed with a soya substitute where
required. No benefit resulted from withholding cows’ milk, indeed symptoms were
more usually associated with this group. Breast feeding, even for a short
period, was clearly associated with a lower incidence of wheeze, prolonged
colds, diarrhoea, and vomiting. It seemed that the duration of breast feeding
was less important than whether or not the child had been breast-fed at all.
Wheezing was both more common among boys than girls (P less than .05) and if
the mother was a smoker. Other environmental features related to wheezing were
social class, month of birth, lack of breast feeding, exposure to dampness,
mould and coal fires, but not to domestic pets nor to the numbers of mites
found in bedding and carpets. Mite exposure was, however, associated with
prolonged colds. Eczema was the only allergic symptom not positively associated
with any environmental factor; moreover, itwas neither associated with a lack
of breast feeding nor with inclusion of cows’ milk in the diet. Eczema was
associated with the incidence of positive skin prick tests and IgE antibodies
to egg white. IgE and IgG4 antibodies were estimated at birth (mothers’ and
cord bloods) and 3 and 12 months later.
TI: Evidence for protection by
breast-feeding against infant deaths from infectious diseases in Brazil
AU: Victora CG,
Smith PG, Vaughan JP, Nobre LC, Lombardi C, Teixeira AM, Fuchs SM, Moreira LB,
Gigante LP, Barros FC
SO: Lancet
2:319-322, 1987.
In a population-based case-control study
of infant mortality in two urban areas of southern Brazil, the type of milk in
an infant’s diet was found to be an important risk factor for deaths from
diarrhoeal and respiratory infections. Compared with infants who were
breast-fed with no milk supplements, and after adjusting for confounding
variables, those completely weaned had 14.2 and 3.6 times the risk of death
from diarrhoea and respiratory infections, respectively. Part-weaning was
associated with corresponding relative risks (RR) of 4.2 and 1.6. The risk of
death from infections other than diarrhoea or respiratory infection was less
clearly associated with breast-feeding (completely weaned, RR = 2.5; partly
weaned, RR = 0.4). Cow’s and formula milk seemed to be equally hazardous. For
deaths due to diarrhoea the increased risk associated with not breast-feeding
was greatest in the first two months of life (RR for completely weaned vs
breast-fed without supplementary milk = 23.3)
TI: Is milk production impaired by dieting during lactation?
AU: Dusdieker
LB, Hemingway DL, Stumbo PJ
SO: American Journal of
Clinical Nutrition 59:833-840, 1994.
To determine the feasibility of a
weight-loss program during lactation, 33 healthy, well-nourished,
breast-feeding women were enrolled. Twenty-two women completed the 10-wk study,
losing a mean (+/- SD) of 4.8 +/- 1.2 kg. Mean energy intake during the study
was nearly 2.25 MJ (538 kcal) below the mean daily baseline intake of 9.64 +/-
2.48 MJ (2303 +/- 592 kcal). The sum of three maternal skinfold thickness,
waist, and hip measurements were significantly smaller (P = 0.0001) at study
completion. Mean daily milk production was 759 +/- 142 mL/d at baseline and 802
+/- 189 mL/d at week 10. The infants gained an average of 21 g/d, or 1.48 +/-
0.40 kg overall. The mean percent fat of milk at baseline and 10 wk was 4.06
+/- 2.15 and 4.00 +/-2.56, respectively. The mean daily nitrogen content of
milk at baseline and study completion was 1.82 +/- 0.32 and 1.62 +/- 27 g/L.
These findings suggest that modest weight loss by healthy breast-feeding women
does not adversely affect either quantity or quality of milk consumed by their
infants.
TI: Maternal weight-loss patterns during prolonged lactation
AU: Dewey KG,
Heinig MJ, Nommsen LA
SO: American
Journal of Clinical Nutrition 58:162-166, 1993.
Weight and triceps-skinfold thickness
were measured until 24 mo postpartum in matched cohorts of women who breast-fed
for > or = 12 mo (BF; n = 46) or < or = 3 mo (FF; n = 39). In the BF
group, breast-feeding frequency and breast-milk energy output were determined
every 3 mo until 18 mo. Weight loss from 1 to 12 mo postpartum was
significantly greater in BF than in FF women (4.4 vs 2.4 kg, P < 0.05), due
primarily to differences in weight loss from 3 to 6 mo. BF mothers had a net
loss in triceps-skinfold thickness whereas FF mothers gained fat at this site
(-0.4 vs 2.4 mm, P < 0.05). Breast-feeding frequency and total time breast-
feeding were related to weight loss in the BF group from 6 to 12 mo. Maternal
weight did not differ significantly between 12 and24 mo in either group. We
conclude that lactation enhances weight loss postpartum if breast-feeding
continues for at least 6 mo.
TI: Acute prolactin and oxytocin responses
and milk yield to infant suckling and artificial methods of expression in
lactating women
AU: Zinaman MJ,
Hughes V, Queenan JT, Labbok MH, Albertson B
SO: Pediatrics
89:437-440, 1992.
Breast-feeding is today the major form of
infant nutrition in the immediate postpartum period. Despite this, recent
trends in modern life-styles have raised obstacles to successful lactation.
These include infant illness and maternal responsibilities outside the home,
both requiring separation from the mother. While the hormonal dynamics of
infant suckling are understood, little is known about the effects of artificial
methods of milk expression. A variety of breast pumps exist in the current US
market which vary considerably in price and effectiveness. To understand better
the ability of these pumps to assist women in the maintenance of lactation, the
current study was undertaken to evaluate their effects on milk yield and
prolactin and oxytocin release when compared to natural infant suckling. Twenty-three
women who were exclusively breast-feeding their infants were randomly assigned
to serially use several pumping methods, as well as infant suckling, with blood
being taken at 10-minute intervals to determine the hormonal responses. The
results reveal variability in the prolactin responses to the artificial pumping
methods, with the greatest responses found with an electric pulsatile pump;
these responses compare favorably with those of natural infant suckling. Other
methods were less successful in causing prolactin elevations. No differences
were seen among the methods in the oxytocin response. The results of this study
demonstrate striking differences in the ability of breast-pumping methods to
produce an acute and sustained prolactin rise in breast-feeding mothers. The
large discrepancies found suggest the need for furtherstudies in to enable
women and health care providers to choose the most appropriate method for milk
expression.
TI: Independent protective effect of lactation against
breast cancer: a case-control study in Japan
AU: Yoo KY,
Tajima K, Kuroishi T, Hirose K, Yoshida M, Miura S, Murai H
SO: American
Journal of Epidemiology 135:726-733, 1992.
A case-control study was carried out to
assess the risk of breast cancer associated with breast feeding in Japan. The
data were obtained in a hospital-based case-control study of 521 women with
breast cancer and 521 controls from January 1988 to December 1989. Statistical
adjustment for potential confounders as well as a likelihood ratio test for
linear trend was done by unconditional logistic regression. Compared with
parous women who had never breast-fed, women with a positive history of breast
feeding had an odds ratio of breast cancer of 0.62 (95% confidence interval
0.37-1.04). The trend of decreasing risk with increasing average months of
breast feeding was statistically significant (chi 2 trend = 4.5, p less than
0.05), while it was was nonsignificant for the number of breast-fed children
borne. Among premenopausal women, a significant linear relation with a
log-transformed term of average months of breast feeding was noted, regardless
of the age of the woman at first full-term pregnancy and parity (chi 2 trend =
5.3, p less than 0.05). The risk was the lowest among premenopausal women who
had ever lactated for 7-9 months (adjusted odds ratio = 0.39, 95% confidence
interval 0.15-0.97). These findings suggest that lactation has an independent
protective effect against breast cancer in Japanese women.
Drug
Abuse / НаркоманиЯ
This issue includes 11 abstarcts on drug abuse in its
various aspects: results from long-term randomized drug abuse prevention
trials, perspectives of the problem of studying drug abuse and how it is
related with HIV/AIDS, infectious diseases, etc.
The abstracts reveal only a small fraction of the
information available on this socially relevant health problem.
В раздела са включени 11 резюмета, третиращи
зло-употребата с упойващите вещества в нейните различни аспекти: резултати от дългосрочни
рандомизирани про-учвания на превенцията на злоупотребата, перспективите на
изследванията на злоупотребата с наркотици и връзката й с HIV / AIDS,
инфекциозните заболявания и злоупотребата с наркотици и др.
Естествено, в този малък обем на информация по този
огромен по своята социална значимост и мащаби проблем не могат да се обхванат
всички негови аспекти.
доц.
д-р Мария Александрова
TI: Long-term follow-up results of a
randomized drug abuse prevention trial in a white middle-class population.
AU: Botvin GJ. Baker E.
Dusenbury L. Botvin EM. Diaz T.
AD: Institute for
Prevention Research, Cornell University Medical College, NewYork, NY, USA.
SO: JAMA. 273(14):1106-12, 1995 Apr 12.
OBJECTIVE: To evaluate the long-term
efficacy of a school-based approach to drug abuse prevention. DESIGN:
Randomized trial involving 56 public schools that received the prevention
program with annual provider training workshops and ongoing consultation, the
prevention program with videotaped training and no consultation, or “treatment
as usual” (ie, controls). Follow-up data were collected 6 years after baseline
using school, telephone, and mailed surveys. PARTICIPANTS: A total of 3597
predominantly white, 12th-grade students who represented 60.41% of the initial
seventh-grade sample. INTERVENTION: Consisted of 15 classes in seventh grade,
10 booster sessions in eighth grade, and five booster sessions in ninth grade,
and taught general “life skills” and skills for resisting social influences to
use drugs. MEASURES: Six tobacco, alcohol, and marijuana use self-report scales
were recorded to create nine dichotomous drug use outcome variables and eight
polydrug use variables. RESULTS: Significant reductions in both drug and
polydrug use were found for the two groups that received the prevention program
relative to controls. The strongest effects were produced for individuals who
received a reasonably complete version of the intervention: there were up to
44% fewer drug users and 66% fewer polydrug (tobacco, alcohol, and marijuana)
users. CONCLUSIONS: Drug abuse prevention programs conducted during junior high
school can produce meaningful and durable reductions in tobacco, alcohol, and
marijuana use if they (1) teach a combination of social resistance skills and
general life skills, (2) are properly implemented, and (3) include at least 2
years of booster sessions.
TI: School drug education programming: in
search of a new direction. [Review]
AU: Lamarine RJ.
AD: Department of
Health and Community Services, California State University, Chico 95929-0505.
SO: J Drug
Educ. 23(4):325-31, 1993.
School
drug abuse prevention programs represent an enormous educational resource.
Recent perceptions of an epidemic of drug abuse among the nation’s youth have
fueled the escalation in expenditures for drug prevention programming. An
important question that needs to be addressed concerns whether broad ranging
drug education efforts directed at all public and private schoolstudents are
efficient and effective uses of available resources? After a brief survey of
the evolution of drug education programming in the U.S., this article examines
recent longitudinal research regarding the antecedents of drug abuse among
young people. Based on this research, suggestions are made for a new approach
to drug education programs which would direct intensive interventions at the
minority of youth who are identifiable in early childhood as particularly
susceptible to problems with drug abuse.
TI: Drug abuse research and HIV/AIDS: a national perspective
from the US.
AU: Schuster CR.
AD: National
Institute on Drug Abuse, Rockville, MD 20857.
SO: Br J
Addict. 87(3):355-61, 1992 Mar.
The National Institute on Drug Abuse
(NIDA), the lead Federal agency charged with research on reducing the demand for
illicit drugs in the US, has actively pursued the associated challenge of
reducing drugs-related HIV transmission. Drug abuse-related spread of the virus
occurs not only through sharing contaminated needles but also sexually to
partners and perinatally from infected mothers to their offspring. Through a
national research and demonstration program, NIDA supports primary AIDS risk
reduction activities focused on identifying effective drug abuse prevention and
treatment strategies. AIDS is increasingly a disease found in women, children,
minorities, and people who live in rural areas. NIDA’s efforts are clearly
responsive to the changing nature of this epidemic. Among the many promising
initiatives currently underway are a medications development program to find
new pharmacotherapies for treating drug addiction; an array of National AIDS
Outreach Demonstration Projects implementing alternative control strategies for
drug abusers not attracted to or successful in drug abuse treatment;
establishment of several treatment research units for designing and conducting
studies on treatment effectiveness; and a variety of programs aimed at
identifying and potentially reducing the risks of prenatal drug use to both
mother and child. Effectivedissemination of our findings is particularly
critical to the overall impact of our research efforts. Collaborative
activities teaming NIDA with a multitude of organizations also addressing AIDS
related issues are designed to provide a synergistic impact on this complex and
multifaceted public health crisis.
TI: The International Catholic Child
Bureau and drug abuse: contributions to drug abuse prevention by a
non-governmental organization concerned with children.
AU: Ruegg F.
AD: International
Catholic Child Bureau, Geneva, Switzerland.
SO: Bull
Narc. 43(1):9-15, 1991.
The present article is an attempt to
demonstrate that a broad-based approach to matters directly affecting children,
with special emphasis on meeting their non-material and spiritual needs, can
effectively contribute to drug abuse prevention, in particular, by promoting
personal values that encourage constructive use of goods and time. The
International Catholic Child Bureau (ICCB) has adopted its approach to drug
abuse prevention, particularly in respect of “street children”, and, through
its vast network of experts and practitioners familiar with intercultural and
interdenominational education, has implemented a number of projects in Africa,
Europe and Latin America, primarily involving the use of therapeutic communities,
workshops and “street educators”. The religious dimension of the work of ICCB
is particularly important because it highlights a fundamental aspect for youth
of all cultures, i.e. integrated preparation for life as responsible members of
the community. ICCB is of the view that it is imperative to provide children
with possibilities for a life that is free of substance dependence, once they
are able to make the right decisions.
TI: RNs and DAs collaborate to prevent drug abuse.
AU: Louie KB.
SO: Nursingconnections. 4(4):5-11, 1991 Winter.
Two unique disciplines have come
together in a large urban community to provide a community-based drug
prevention program for children: Pupils, Lawyers, and Nurses (P.L.A.N.) Against
Drugs. This unique relationship brings two sets of expertise to better respond
to the complex problem of drug abuse. The program approaches drug abuse
prevention by focusing on law enforcement and nursing as career options for
inner city children. Cooperation was emphasized from the initial planning
stages through project implementation. Other contributors to this program
include school district leaders, teachers, community leaders, representatives
from the state division of substance abuse, nursing faculty, and district
attorneys. The program has received international and national recognition for
its efforts. This paper describes the advantages of the collaborative approach
to a complex problem.
TI: Infectious diseases and drug abuse. Prevention
and treatment in the drug abuse treatment system. [Review]
AU: Haverkos HW.
AD: Division of
Clinical Research, National Institute on Drug Abuse, United States Public
Health Service, Rockville, Maryland 20857.
SO: J Subst Abuse
Treat. 8(4):269-75, 1991.
Several communicable infectious
diseases, including AIDS, hepatitis B infection, gonorrhea, syphilis, and
tuberculosis, are increasing among drug abusers. Drug abuse treatment programs
may be ideal sites to identify those infections and initiate and maintain
appropriate medical management. This paper reviews the epidemiology of those
infections among drug abusers in the USA, presents rudimentary aspects of
medical management of selected infectious diseases, and discusses the need to
integrate infectious diseases, drug abuse treatment, and public health
approaches if weare to reverse, or at least stabilize, the trends of those
diseases. [References: 32]
TI: DIADS: computer-based system for development of school
drug prevention programs
AU: Bosworth
K. Yoast R.
AD: Indiana
University.
SO: J Drug
Educ. 21(3):231-45, 1991.
The Drug Information, Assessment and
Decisions for Schools (DIADS) is a computer-based information and decisions
support system for the development of school drug abuse prevention programs.
DIADS provides access to a cost-effective planning resource that has
information to programs about alcohol, other drugs, and prevention. Also, DIADS
helps the school assess the effectiveness of its current prevention efforts
using an expert-generated school assessment model containing fourteen factors. Fdedb‘ck from the assessment provides suggestions
for improvements in current prevention programs. DIADS guides the
selection of future activities and helps in program planning. Pilot test of
DIADS at several sites indicates school personnel find the information on DIADS
helpful, timely and easy to access.
TI: Stage theory and research on tobacco,
alcohol, and other drug use.
AU: Werch-CE;
Anzalone-D
AD: Center for
Alcohol and Drug Abuse Prevention and Health Promotion College of Health,
University of North Florida, USA.
SO: J-Drug-Educ.
1995; 25(2): 81-98
The purpose of this article was to
examine the conceptual and empirical foundations of individual drug use stage development
and progression related to tobacco, alcohol, and drugs. This review indicated
that while greater acceptance of the idea that drug use is a complex process,
the majority of stage conceptualizations suffer from significant limitations.
Although limited, research conducted to date is supportive of the existence of
intra-drug use stages of acquisition for cigarettes and other drugs. Research
examining inter-drug use progression among youth supports the idea of a
generally invariant sequence at a macro-sequential level, involving nonuse to
legal drug use, marijuana use, and finally other illegal drug use.
TI: Parent participation in an adolescent drug abuse
prevention program.
AU: Cohen-DA;
Linton-KL
AD: Louisiana
State University Medical Center, New Orleans, USA.
SO: J-Drug-Educ.
1995; 25(2): 159-69
This study reports the level of
participation of parents in a parent-targeted school-based drug prevention
program, the differences between students whose parents participate and those
who don’t, and the implications for involving parents in future drug prevention
programs. Among 1761 eligible seventh grade families, 1263 students (72%) and
1142 parents (65%) completed surveys assessing the quality of parent-child
relationships as well as tobacco and alcohol use. Ten percent of eligible
families attended at least one of the evening sessions. Compared to students
whose parents completed the survey, students whose parents did not complete a
survey were more likely to report they used tobacco, had more friends who used
substances, were monitored less by their parents, had more risk-taking
behaviors, had lower grade-point averages, and their parents had higher rates
of tobacco and alcohol use. Parents who attended evening sessions had the
lowest rates of tobacco use and reported spending the most time with their
children. Parent-targeted drug prevention programs may stigmatize attending
parents and may be unlikely to attract the highest risk families.
TI: Anabolic-androgenic steroids. Current
issues.
AU: Yesalis-CE;
Bahrke-MS
AD: Health Policy
Science, College of Health and Human Development, Pennsylvania State
University, University Park, USA.
SO: Sports-Med.
1995 May; 19(5): 326-40
The use of drugs to enhance physical
performance has been observed for thousands of years. Today, individuals
continue to use a variety of substances, including anabolic-androgenic
steroids, in the hope of enhancing their performance and appearance. Rumours
persist regarding the incidence of the nonmedical use of anabolic steroids by
athletes and nonathletes: however, true estimates are now available based on
the results of systematic surveys. Although the vast majority of the athletic
community accepts that anabolic steroids enhance performance and appearance,
the extent to which this occurs and the factors influencing such effects remain
incompletely understood and documented. Refinement of our knowledge of the
ergogenic effects of anabolic steroids is not without merit; however, the
existing scientific evidence coupled with an overwhelming number of anecdotal
accounts argues against devoting significant resources to this area of
investigation at present. The short term health effects of anabolic steroids
have been increasingly studied and reviewed, and while anabolic steroid use has
been associated with several adverse and even fatal effects, the incidence of
serious effects thus far reported has been extremely low. The long term effects
of anabolic steroid use are generally unknown. Unfortunately, the lack of
scientific information on long term health effects has impeded, if not
precluded, the formation of effective health education and drug abuse
prevention strategies. Consequently, efforts should be expanded in the areas of
prevention and education.
TI: Process evaluation of Nebraska’s Team
Training Project.
AU: Scott-DM;
Merkel-PA; Barlow-TW
AD: Department of
Pharmacy Practice, University of Nebraska Medical Center, Omaha 68198-6045.
SO: J-Drug-Educ.
1994; 24(3): 269-79
BACKGROUND. A process evaluation of the Nebraska
Drug Free School/Community Residential Team Training Project is described. This
training project utilizes a “system approach” in the formation and
implementation of localized strategic (action) plans targeting alcohol and
other drug (AOD) abuse prevention. METHODS. In June of 1990, training
participants completed a pre-post survey in conjunction with the four-day
training. The majority of the participants (51.2%) were teachers, 19.2 percent
were parents, 13.6 percent administrators, and 9.6 percent were counselors.
RESULTS. Although the overall attitudes of the participants (N = 125) were
positive initially, they became even more so by the end of the training (N =
121). Prior to training participants felt they could have a significant impact
on their local AOD abuse problem, and this attitude became more positive by the
completion of training (p < 0.05). CONCLUSIONS. The Nebraska team training
process immerses team members in an active planning process allowing teams to
develop a plan of action for their school and community. During this process,
participants experience a positive growth in attitudes reflecting not only the
training experience itself, but even more importantly their ability to
meaningfully affect AOD abuse and related destructive behaviors in their homes,
schools, and community.
Завършени проекти по програма "Решаване на проблеми
за по-добро здраве"
СКРИНИНГОВО ПРОУЧВАНЕ НА УПОТРЕБАТА И ЗЛОУПОТРЕБАТА С
ПСИХОАКТИВНИ ВЕЩЕСТВА СРЕД ПОДРАСТВАЩИТЕ
Александрова
М., Д. Киров, ВМИ - Плевен
Катедра “Психиатрия и медицинска психология с ЦПЗ”
Асоциация
за профилактика на наркоманиите - Плевен
Употребата
и злоупотребата с психоактивни вещества сред подрастващите се превърна в социално
значим проблем през последните 5-6 години в нашата страна.
Причините
за това явление са обусловени от многобройни социални, икономически и политически
фактори.
Като
явление от обществения живот явлението наркомания е много кратко във времето.
Българските наркомани не са имали време да узреят. Те са много млади и
неразвити социално и емоционално, затова оказват съпротива срещу всякакви
колективни и индивидуални интервенции. Това е големият проблем. Значително част
от младите хора отхвърлят или не приемат старите ценности -привързаност към
семейството, любов към труда и т.н. Те утвърждават свои норми на поведение и
живот, които отговарят на тяхната ценностна система. Известно е, че младите
хора днес растат и узряват физически и психически по-бързо, а времето на
тяхната социална зависимост и несамостоятелност се удължава. Получава се
парадокс, който довежда до различни форми на негативистично поведение, насочено
към семейството, реда и обществото. Така се създават условия за образуване на
малки неформални групи, като много често асоциалното поведение на участващите в
тях е свързано със злоупотреба с наркотици. Но наркоманната епидемия сред младежта
има и редица други предпоставки. Важно значение имат генетически и
психологически причинни фактори. Безспорно обаче, най-голямо е значението на
социалните фактори. Сред тях на първо място трябва да се изтъкне сега
съществуващата възможност без сериозни затруднения да се набавят желаните
психотропни вещества.
Важна
характеристика на наркоманния проблем у нас понастоящем е бързото му “взривоподобно”
разрастване. Друга характеристика, която ни отличава от Европа например е
рязкото спадане на възрастовата граница - средна възраст на употребяващите
хероин е 14 - 16 години, на медикаменти - 12 - 14 години, а на летливи разтворители
б /лепила/- по-малка от 12 години. За страните от Западна Европа средната
възраст е над 25 години.
За
да установим приблизителните мащаби на употребата и злоупотребата с
психоактивни вещества сред подрастващите проведохме скринингово анкетно
проучване на 1200 ученика на възраст 15 - 17 години в различни училища на
Плевен и региона. Юношите попълваха анонимен въпросник с 15 въпроса, всеки един
с по 5 възможни отговора.
Проучени
бяха социодемографските показатели, микросоциалните условия, психологичните и
личностните особености на младежите.
От
всички анкетирани 10.5% заявяват, че по един или друг повод са опитвали опиати,
а 7.8% отговарят, че употребяват психоактивни вещества.
Резултатите
показват, че в 51% от случаите поводът за вземане на упойващи вещества е бил любопитството.
За 44 % от анкетираните обаче, това е начин за бягство от действителността,
което буди основателна тревога и много размисъл.
Според
изследваните една от най-важните причини за употребата на наркотици трябва да
се търси в семейството. Очертават се проблемите - занижен или липсващ
родителски контрол, отчуждение между родители и деца, финансови проблеми.
Налице са данни за наличие на напрежение в отношенията между подрастващите и
техните родители, което лесно прераства в конфликт между поколенията.
Проблемното общуване в семейството често става повод неукрепналите психически
младежи често да търсят спасение в наркотиците.
Друг
извод, който се налага е, че приятелската среда заема централно място във
всекидневния живот на учениците. Анкетираните са единодушни, че първият прием
на опиати е станал под влияние на приятелите. Обикновено това е ставало по
време на сбирка, екскурзия, в дискотеки и т.н. При 66% от младежите нито един
от приятелите им не приема наркотици, при 33 - само някои от приятелите им
вземат епизодично, а само в 1% - всичките им приятели вземат и в момента наркотици.
За
юношите, попаднали под влияние на опиатите е характерно, че дават предпочитание
на забавленията, личната свобода, секса, парите, любовта, а на последно място в
ценностната им система е отношението към образованието, труда семейството. Тази
категория младежи не се интересуват от спорт, изкуство, нямат цел в живота.
Прави
впечатление, че първата среща с дрогата е на възраст 14 - 15 години. Мотивите
за първата употреба на наркотици според анкетираните са следните:
-
на първо място - 51% - любопитството и желанието да се изпита еуфория.
-
на второ място - 44% - това е липса на перспектива в живота и начин да избягат
от действителността.
-
на трето място - 3% идва стремежът за подражание на приятели и идоли.
-
на четвърто място - 2% - посягането към дрогата е случайно, поради непознаване
на вредното въздействие върху здравето и организма.
Честотата
на вземане при младежите, употребяващи дроги е както следва:
-
при 76% - само при събиране с приятели.
-
при 12% - веднъж седмично.
-
при 11.7% - няколко пъти седмично.
Относно
вида на употребяваните психоактивни вещества се доказа, че 64.3% от
подрастващите са използвали успокояващи медикаменти /бензодиазепини/, 28.6% -
летливи разтворители, 21.4% - преработени упойващи вещества и 14.3% -
комбинирани препарати.
В
85.7% от случаите, когато се употребяват наркотици пътят за приемането им е
през устата и горните дихателни пътища. Само 14.3% от изследваните се
инжектират с упойващи вещества.
Особено
важно е, че 67.5% от изследваните свързват инжектирането на наркотици с възможността
от заразяване с HIV инфекция и заболяване от СПИН.
Интерес
представляват данните за начина на снабдяване с психоактивни вещества. Преобладаващото
мнозинство от употребяващите - 70% се снабдяват от черния пазар, 18% от
неизвестен източник, 12% - с подправени рецепти. Налага се изводът, че е
завишен интересът от страна на наркопласьорите към младите хора и занижен
контролът в аптечната мрежа.
На
въпроса какви мерки предлагат самите анкетирани за ограничаване
разпространението на наркотици се получиха интересни предложения:
-
27% от анкетираните искат повече информация за вредата от употребата на опиати.
Те искат да има повече видео- и телевизионни филми на здравна тематика.
-
17% настояват да се предприемат по-строги мерки срещу разпространителите, вкл.
и смъртно наказание.
-
9% - да се предприемат законодателни и съдебни мерки срещу институциите,
легализиращи и подпомагащи пласирането на дроги.
-
6% - да се разработят нови форми за занимание на учениците в свободното им
време.
-
6% - предлагат да се обогати и разшири базата за спортуване на младежите, за
развитие на способностите и талантите на децата.
-
За 5% е от значение да се подобрят условията на живот в техните семейства и се
създадат условия за пълноценна реализация на младите хора след завършване на
образованието им.
В
заключение може да се каже, че обектът и мащабите на употребата на упойващи
вещества застрашително бързо нараства, особено сред младите хора в обществото.
Това изисква навременни превантивни действия за ограничаване търсенето и
разпространението на наркотици, както от страна на държавните институции, така
и от обществото като цяло.
ОБУЧЕНИЕ НА БОЛНИ С БРОНХИАЛНА АСТМА С ОГЛЕД ЕФЕКТИВЕН
КОНТРОЛ НА ЗАБОЛЯВАНЕТО
Бронхиалната
астма е често заболяване, което засяга хората от всички възрастови групи. Особено
засегнати са урбанизираните райони.
Истинската
честота на бронхиалната астма трудно може да се определи. Причините за това са
различните диагностични критерии, неточната регистрация, самолечението на част
от болните.
Съвременни
големи проспективни проучвания показват нарастване честотата на бронхиалната
астма (БА) в цял свят. Освен това се установява и по-тежко протичане. Това нарастване
на морбидитета и тежестта на БА увеличават финансовото натоварване на
обществото. Нарастват не само преките медицински разходи (лечение, спешна
помощ, консултации и др.), но и непреките такива (отсъствие от работа и
училище, време за пътуване и чакане, намалена работоспособност, нарушен семеен
микроклимат и др.).
Плевенският
регион е разположен в Централна Северна България. Климатът е континентален с
горещо сухо лято и продължителна студена зима. Регионът е силно
индустриализиран (петролна рафинерия, циментови заводи, текстилни и
машиностроителни заводи и пр.). Това определя голямото замърсяване на околната
среда,поради липсата на средства за пречиствателни съоръжения. През последните
години се понижи контрола върху замърсяването, поради пренебрегване на въпроса
от обществото.
Рязко
нарасна употребата на цигари, особено сред подрастващото поколение и жените.
Безработицата и постоянният стрес тласкат хората към нискохигинен начин на
живот.
В
условията на градска пренаселеност, замърсяване на околната среда,
тютюнопушене, високи цени на медикаментите се създават условия за голям брой
респираторни инфекции и непълноценното им излекуване. Здравната мрежа е също в
състояние на стрес: лоши условия на труд, минимално финансиране, ниски заплати,
лошо обучение, липса на всякакви здравни програми. Това определя липсата на
мотивация в здравния персонал и снижава нивото на медицинското обслужване.
В
тези условия броят на болните от бронхиална астма в Плевенския регион се
увеличава. Нараства тежестта на протичане на заболяването.От тук възниква
необходимостта от създаване на прости, евтини и социално eфективни програми за
обучение на болните от бронхиална астма.
Главна
цел на проекта е да се обучат болните от бронхиална астма как да контролират
своето заболяване с цената на минимални обществени и лични разходи. По своята
същност това е едно образователна програма.
Като
първа стъпка бе разкрит т.нар. “АСТМА” кабинет във II градска поликлиника
Плевен. Оборудване: компютър със специална програма за регистриране на болните
с бронхиална астма (БА); апарат за изследване на дишането (Spirocomp);
телефонен апарат със автоматично записващо устройство (секретар); средства за
инхалиране. Кабинетът се обслужва от 6 лекари специалисти по белодробни
заболявания и един студент по медицина. Започна се с 5 работни дни - по 4 часа
следобед. С оглед оптимално натоварване се премина на приемни дни 3 пъти
седмично по 2 часа. Кабинетът започна работа през м.май 1995 г. Болните с БА се
регистрират, измерват се функционалните им показатели, преглеждат се. От тук
започва и новото в работата ни: всеки болен индивидуално се обучава: същността
на заболяването му, факторите които предизвикват пристъпи, необходимото
лечение, поведение по време на пристъп. Особено внимание се обръща на
правилната техника на инхалиране с оглед ефективното използване на вдишвания
медикамент. За целта бе заснет филм с демонстрация на правилно инхалиране.
Видеокасетата бе размножена в 100 копия, които се предоставят на болните
безплатно. Впрочем помощта, която болните получават в “АСТМА” кабинета е
напълно безплатна. Освен това болните получават при облекчени условия
спомагателни уреди за вдишване (спейсъри) и джобни апарати за измерване на дишането (пийкфлоуметри). Бяха разработени
дневни карти, на които те записват измерените стойности на дишането. Там са
отбелязани и указания за действие в спешни ситуации. Отделно бе заснет и филм с
изказвания на болни преди и след включване в програмата. Към този момент в
компютъра са регистрирани около 1000 болни от БА, които са били индивидуално
обучени по време на посещенията си. Болните се насърчават да идват в кабинета
или да се обаждат по телефона. Обработените досега данни посочват, че
контролираните от нас болни получават по-рядко пристъпи, по-рядко посещават
“Бърза помощ” и постъпват в болница, имат по-малко дни отсъствия от работа или
училище, харчат по-малко пари за лечение. В крайна сметка това е
социално-икономическият ефект от нашите усилия.
Друго
направление на тази програма е работата с лекарите на ниво първична помощ. Бяха
проведени серия от срещи с тях Плевен, Враца, Троян, Тетевен, Кърджали,
Хасково. Представени бяха новостите в лечението на БА. Показани им бяха заснетите филми, раздадени материали,
помощни средства. За Плевен и региона бе установено много полезно взаимно сътрудничество.
Сега се прави опит да се приложи еднакъв терапевтичен подход в Центъра за
Спешна Медицинска Помощ Плевен. Радостно е, че подобни кабинети се разкриха с
наша помощ във Враца и Видин. Те използват сходен модел на работа.
Като
част от проекта е и сътрудничеството ни с фармацевтичните фирми, производители
на съвременните лечебни средства. Предоставените мострени препарати се раздават
с предимство на пенсионери, безработни, учащи. Освен това от тях получаваме и
ценна помощ при организирането на споменатите срещи.
Постигнатите
от нас резултати намират своевременно отражение в местните и централни средства
за масово осведомяване.
Изминат
е половината път от предварително начертания. Удовлетворени сме от постигнатото
и ще продължим, съзнавайки ползата от нашия труд за болните и обществото.
Координатор на проекта: д-р Явор Иванов, п.к. 1018,
Плевен 5800, тел. 33340
Участници: д-р Валери Андреев, д-р Пламен Павлов, д-р
Павлина Глоговска, д-р Цаня Попова,
д-р Стела Вулова.
ПРОФИЛАКТИКА И КОНТРОЛ НА ОСТРИЯ МИОКАРДЕН ИНФАРКТ
М. Цекова
Кардиологична клиника
ВМИ - Плевен
В
САЩ и в повече от западноевропейските страни смъртността от исхемична болест на
сърцето достига своя максимум през шестдесетте години на нашия век, след което
се наблюдава постоянна тенденция към снижаването й. През последните 40 години е
постигнат голям напредък в борбата със специфичните ефекти на ИБС. Например
през 1950 година смъртността в САЩ от ОМИ е 226,4 на 100 000 души, а през 1987
- 124,1 на 100 000 души население. Тази тенденция към снижаване на
заболеваемостта и смъртността от ОМИ е постигната чрез промяна в стила на живот
и хранене, ограничаване на тютюнопушенето, контрол на артериалната хипертония,
подобряване на доболничните грижи, създаване на интензивни кардиологични
отделения, въвеждане на фибринолитичната терапия в острата фаза на ОМИ. Според
данни на СЗО през последните години темповете на заболеваемостта от ИБС в
източноевропейските страни се повишава, като България е на четвърто място в
света. Според данни на СЗО смъртността от ОМИ в България е била общо за мъже
102,1 на 100 000 хил. души и за жени 43 на 100 000 души население през 1990 г.,
а за 1991 г. съответно 109,5 за мъже и 44,8 на 100 000 за жени, т. е. само за 1
година смъртността от ОМИ за мъже се повишава със 7,4 и за жени с 1,8 на 100
000 души население.
Проблемът на настоящия проект е нарастващата
заболеваемост и високата смъртност от ОМИ в България през последните години.
Цели:
За
изясняване на проблема си поставихме следните цели:
1.Проучване
честотата, разпространението и динамиката на заболеваемостта, хоспитализацията
и смъртността от остър миокарден инфаркт /ОМИ/ в региона на Плевенски окръг с
население 342 000 души за три годишен период.
2.Установяване
продължителността на доболничния период на ОМИ и съставящите го 3 фази /от
появата на болката до повикване на лекаря, от повикване на лекаря до първия
медицински преглед и от първия медицински преглед до хоспитализацията/.
3.Проучване
честотата на някои рискови фактори при болните с ОМИ.
4.Разработване
на материали и здравна програма за контрол на основните рискови фактори за ОМИ.
5.Популяризиране
на резултатите и повишаване информираността на населението и на застрашените от
ОМИ, с цел намаляване на заболеваемостта от исхемична болест на сърцето и
своевременно започване на лечението на болните от ОМИ.
Резултати:
За
периода 1990 - 1994 година заболеваемостта от ОМИ в региона постоянно се
покачва. От 1990 до 1992 се наблюдава рязък скок в заболеваемостта от ОМИ, като
през следващите 2 години тревожната тенденция към повишаване на заболеваемостта
от ОМИ се запазва.
Заболеваемост от ОМИ в региона на Плевенски окръг
/1990-1994/
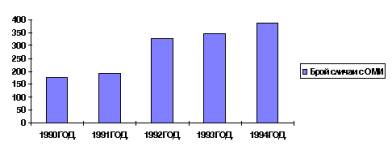
Анализираха се данните за заболеваемостта и смъртността
от ОМИ в общините в региона на бившия Плевенски окръг за 1993 и 1994 година.
Смъртността от ОМИ е твърде висока. Например за университетска болница - Плевен
е 17,0% и 22,4%, за община Червен бряг - 22,7% и 50%, за община Гулянци - 51,1%
и 84,6% съответно за 1993 и 1994 г. Цитираните данни показват недопустимо
висока смъртност от ОМИ за една европейска държава, като се има предвид, че
смъртността от ОМИ в Западноевропейските страни и в САЩ през последните години
е снижена до 6,8%-10,2%.

Аналогични са данните за заболеваемостта и смъртността от
ОМИ през 1994 г. по общини, както се вижда от следващите таблица и графика.
Заболеваемост
и смъртност от ОМИ за 1994 година по общини
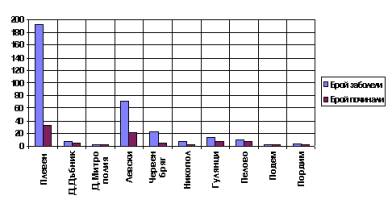
Анализирани
са приетите болни с ОМИ за лечение в МУ - Плевен. За периода 1990-1994 са
приети 1090 болни с ОМИ, като само при 136 от тях е проведена фибринолитична
терапия със стрептаза в първите 6 часа.
Данни за проведена фибринолиза при болните с ОМИ в
МУ-Плевен за периода 1990-1994 година. През 1994 г. само 43 болни са получили
стрептаза-18,5%
Данни
за проведена фибринолиза при болните с ОМИ в МУ - Плевен за периода 1990-1994 година
През 1994 г. само 43 болни са получили стрептаза-18,5%

Известно
е, че своевременната хоспитализация на болните с ОМИ има решаващо значение за
провеждане на фибринолитична терапия при ОМИ. При болните третирани със
стрептаза смъртността е значително по-ниска - 7,2%, докато при болните, при
които не е проведена фибринолиза смъртността е 18-25%.
За
установяване продължителността на доболничния период, бяха попълнени анкетни
карти на 232-ма болни приети на лечение в интензивно кардиологично отделение,
ВМИ-Плевен през 1994 година. Установи се, че средната продължителност на първата
фаза на доболничния период /от появата
на симптоматиката до взимане на решение за търсене на лекарска помощ/ е твърде
голяма и при 133 болни /57,4%/ превишава 6 часа. Интерес представлява фактът,
че продължителността на тази фаза не зависи от образоваността на пациентите, т.
е. информираността на населението за алармиращите симптоми на заболяването е
крайно ограничена. Средната продължителност на втората фаза на доболничния
период /от търсенето на медицинска помощ до първи лекарски преглед/ е между 1 и
2 часа при 187 болни /80,6%/. Налага се изводът, че организацията на спешната
медицинска помощ не е перфектна. Продължителността на третата фаза /от първия
лекарски преглед до хоспитализацията на болния с ОМИ/ е средно 1 ч. и 30 мин.
при 192 болни /82,7%/. Тази фаза би могло също да бъде скъсена при своевременно
диагностициране на заболяването.
Изводът
е, че е необходима широка здравна просвета на населението и значително
подобряване на организацията на спешната медицинска помощ с оглед своевременна
хоспитализация на болните с ОМИ и провеждане на фибринолитична терапия, което
ще доведе до снижаване на смъртността в острия период. При 43 от
хоспитализираните 232-ма болни с ОМИ за 1994 г. в интензивно кардиологично
отделение, е проведена фибринолитична терапия. Трима от тези болни са починали, т. е. смъртността в групата болни,
третирани със стрептаза е 6,9%. От 189-те болни, при които не е проведена
фибринолитична терапия са починали 49, смъртността при болните с ОМИ нелекувани
със стрептаза е 25,9%.
Проведени
са анкетни проучвания на тези показатели в община Левски, Малчика, Козарбелене,
Гулянци и други общини. Установява се още по-дълъг доболничен период и
по-висока смъртност през острия период, както се вижда на гореизложените
таблици.
Проучи се честотата на някои рискови фактори за ОМИ при
приетите 232 болни в интензивно кардиологично отделение, ВМИ - Плевен през 1994
година.
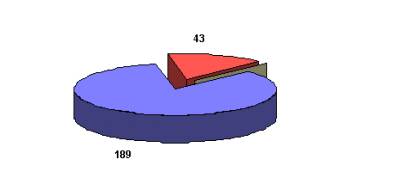
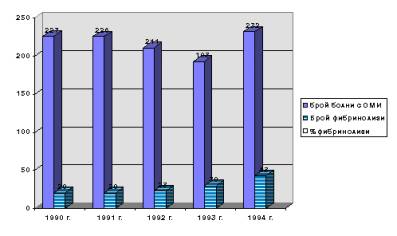
Върху тютюнопушенето и затлъстяването трябва да се
въздейства чрез широка масова здравна просвета и посредством личното поведение
на лекаря в обществото
Болните
с артериална хипертония и захарен диабет са също високорискова група, върху
която трябва да се въздейства чрез широка информираност на населението относно
необходимостта тези заболявания да се лекуват системно с медикаменти и диета.
Бяха
изнесени здравни беседи в завод “Чугун” - Плевен, в ТПК - “Мара Денчева” -
Плевен, в Козарбелене, в Малчика, за необходимостта от здравословен начин на
живот и хранене. Изнесени са лекции за поведението на лекаря от Бърза медицинска
помощ при третирането на ОМИ и неговите най-чести усложнения в ЦСМП гр. Левски.
Разработена е брошура за алармиращите симптоми на ОМИ, също и с препоръки за
здравословен начин на живот, която се отпечата и се разпространява чрез
консултативен кардиологичен кабинет при ВМИ - Плевен. Привлякоха се средства от
Регионалния център по здравеопазване в Плевен за отпечатване на разработената
брошура за ОМИ и разпространението и чрез трите поликлиники в град Плевен.
Осъществиха се 3 радиопредавания по местното радио, публикуваха се материали в
местната преса.
В
заключение:
1.В
Плевенски окръг съществува тенденция към повишаване заболеваемостта от ОМИ.
2.Смъртността
от ОМИ е висока, изключение има само при малката група фибринолизирани болни.
3.Профилактиката
е основен фактор за намаляване на заболеваемостта от ОМИ.
4.От
жизнено важно значение е промяната в стила на живот.
5.Личното
поведение определя степента на риска от ИБС.
6.Ролята
на клиничния лекар е:
-
разпознаване и лечение на рисковите фактори и ОМИ
-
водеща роля в обществената просвета
- лично поведение на лекаря.
Необходимо
е да се помогне на хората да изберат по-здравословен начин на живот чрез широка
здравна информираност, да се определи високорискова група и да се въздейства
върху нея чрез информация и медикаменти.
За
успешното третиране на ОМИ съществено е да се скъси доболничния период чрез
ефективна организация на спешната помощ.
За
проследяване на резултатите от разработените и проведени здравно-просветни
мерки ще е необходим по-дълъг период - 3-5 години, поради което бе прието
продължение на проекта.
Клуб ФОО - Плевен
д-р М. Цекова, инж. Р. Русев
д-р В. Томова, д-р С. Томов
д-р К. Енчев
СъобщениЯ на координатори на действащи проекти СЪЗДАВАНЕ
НА КОЛЕКТИВИ “ПРИЯТЕЛИ НА КЪРМАЧЕТО”
координатор
на проекта: д-р Ваня Недкова- гл. aс. в
кат. “Детски болести”- ВМИ Плевен
Организирано
е обучение на 20 акушерки и медицински сестри от женските и детските консултации
по проблемите на кърменето, предимствата на естественото хранене за здравето на
детето и методите з стимулиране на кърменето, както и неблагоприятното влияние
на тютюнопушенето и психичните натоварвания върху кърменето.
Проучено
е храненето на двумесечните деца от гр. Плевен през 1995 г. и резултатите са
сравнени с данните от 1996 г. Установихме увеличение на процента на естествено
хранените деца от 50 % за 1995 г. до 85 % за 1996 г. Резултатите са изнесени на
Национална конференция по проблемите на храненето - гр. Варна, септември 1996
г. и са представени за публикация в сп. “Педиатрия”.
Изработен
е работен фиш за индивидуална работа с майките-кърмачки.
Публикувана
е статията “Кърменето на децата - изключително важен фактор за развитието им”
във вестник “7 дни в Плевен” - 15-21.II. 1996 г., стр.3.
Определени
са два часа седмично за консултации по проблемите на кърменето.
ПРОФИЛАКТИКА НА РЕСПИРАТОРНИТЕ ИНФЕКЦИИ ПРИ БОЛНИ С
БРОНХИАЛНА АСТМА С RESPIVAX И ПРОТИВОГРИПНА ВАКСИНА
д-р Антоанета Кърчева, клиника по
пулмология - ВМИ - Плевен
I. ВЪВЕДЕНИЕ:
Бронхиалната
астма (БА) е хронично заболяване, което засяга всички възрастови групи. През
последните години то се нареди сред най-сериозните социално значими заболявания.
Тенденцията в развитите страни: увеличаване на честотата, тежестта и засягане
на по-млади възрастови групи,се наблюдава и в нашата страна. Често първата
изява на заболяването се провокира от респираторна инфекция.От друга страна
бактериалните и вирусните инфекции на дихателните пътища на фона на развила се
вече БА почти задължително водят до развила се вече екзацербация на заболяването,
употреба на антибиотици, лекарски прегледи, посещения на Бърза помощ,
хоспитализации, отсъствия от училище и работа. Този факт, съчетан често с
неправилния контрол на заболяването, води до увеличаване на финансовото
натоварване на обществото.
Плевенският
регион е разположен в Централна Северна България. Климатът е континентален с
горещо сухо лято и продължителна студена зима. Регионът е силно
индустриализиран. В условията на градска пренаселеност и замърсяване на
околната среда се създават условия за голям брой респираторни инфекции и
непълноценното им излекуване и оттам за нарастване тежестта на протичане на БА.
От
друга страна поради ниския жизнен стандарт (безработица, ниски заплати, високи
цени на медикаментите) голяма част от обществото реагира неадекватно на своите
заболявания (нисък комплайънс).
В
здравната мрежа липсва единен подход към заболява-нето. В момента се изработва
Национален консенсус за лечение на БА. Предстои неговото практическо въвеждане
и приложение на всички нива.
II. СЪЩНОСТ НА ПРОБЛЕМА:
Често
наблюдаван факт в клиничната практика е изострянето на бронхиалната астма
няколко дни след началото на вирусна или бактериална инфекция. По данни на Ж.
Милева (1994) вирусни агенти се изолират в около 50-60 % от децата с изострена
астма. При възрастни астматици с въвеждането на нови методи напоследък
идентификацията на вирусите нарасна до 54 %. В този смисъл пренасочването на
средствата от квалифицираната медицинска помощ на екзацербациите към
профилактични мероприятия, които да ги предотвратяват, биха имали съществено
значение за контрола на заболяването.
Предлагаме
профилактична програма за предотвратяване на езацербациите, провокирани от
инфекциозни агенти, чрез препоръчителна имунизация срещу грип и прилагане на
полимикробния имуностимулатор Respivax.
В програмата ще бъдат включени две групи болни: 70
възрастни болни от кабинета “Астма” на ФБЗ и 30 юноши на възраст от 15 - 18
години, набрани чрез училищните лекари. Идеята за втората група се породи от
факта, че възрастовата група 15 - 18 години е най-слабо наблюдаваната и изследваната
в здравен аспект. От друга страна по средно статистически данни за Европа БА е
най-често срещаното хронично заболяване в детско-юношеската възраст. Боледуват
10-12 % от децата.
В
рамките на две години на болните от двете групи ще бъдат правени имунизации
против грип и ще бъде прилаган Respivax. Целта е да се проследи как ще се
отрази прилагането на последните върху хода на заболяването, като нашето
желание е с минимални обществени разходи да се даде възможност на тези болни да
водят пълноценен живот.
Наблюденията
ни до този момент върху болни от БА от Плевенския регион показват, че само
незначителна част от тях са правили препоръчителни имунизации поради
непознаване на ваксините от самите болни или от лекуващите лекари.
ДА ПРЕДПАЗИМ ДЕЦАТА ОТ ОТРАВЯНЕ
Д-р
Бойко Шентов, к.м.н.
През
последните години зачестяват случаите на отравяне сред малките деца. Почти
ежедневно в Клиниката по Детски болести на Медицинския Университет постъпват
деца по повод отравяне - най-често с лекарства, селскостопански и битови
отрови. Инцидентите стават обикновено вкъщи и основните причини за възникването
им са неправилното съхраняване на медикаментите и другите токсични вещества,
недостатъчният надзор над децата, по-рядко грешки при даване на лекарство. За
предотвратяване на тези инциденти е необходимо спазването на някои общодостъпни
препоръки:
1.
Лекарствата и другите потенциално токсични вещества вкъщи да се съхраняват на
недостъпно за детето място, нависоко, най-добре в заключен шкаф.
2.
Лекарствата с изтекъл срок на годност да се изхвърлят своевременно.
3.
Всички препарати да се съхраняват по възможност в оригиналните си опаковки и да
бъдат надписани. Честа практика е опасни отрови като сода каустик или
фосфоорганични препарати да се държат в бутилки от безалкохолни напитки.
4.
Тъй като децата имитират възрастните, добре е да се избягва приемането на
лекарства пред тях.
5.
Да не се наричат лекарствата “бонбони”.
7.
Преди да се даде лекарство на детето да се прочетат етикетът и дозировката, ако
е тъмно да се запали лампата.
8.
Децата да не остават без надзор от възрастен.
Добре
е тези препоръки да се имат предвид и когато децата са поверени на грижите на
баби и дядовци, които по-често приемат разни медикаменти.
Спазването
на тези елементарни правила би могло в значителна степен да предпази малкото
дете от понякога смъртоносно отравяне.
ИнформациЯ - проекти в ход
1.
Обучение на пациенти за използване на кислород в домашни условия. За Европа
хроничната обструктивна белодробна болест (ХОББ) е третата причина за
смъртност. Заболяването е най-честият фактор, който води до развитието на
хронична дихателна недостатъчност. Заболяването води до ранна инвалидизация и
смъртност.
Основно
средство за забавяне хода на заболяването и съпътстващите го усложнения е
кислородолечението. По предварителна оценка от данните на сектора по интензивна
терапия от Пулмологична клиника - гр. Плевен, броят на болните, които ще имат
нужда от кислородотерапия за тригодишен период е около 300.
Ето
защо, естествено възникна идея за проект, основна цел на който е да се приложи
за първи път в България системен подход към болните с ХОББ и дихателна
недостатъчност: кислородолечение, инхалаторно лечение и дихателна
рехабилитация. Набраният опит да послужи за основа на подготовка на нормативна
уредба за продължително лечение с кислород в домашна обстановка.
Проектът
се осъществява едновременно като експериментален, образователен и с елементи на
профилактика. На първият етап бяха планирани - подготвителен етап и мероприятия
с целева група за кислородолечение, а на втория - мероприятия с по-обемна целева група и организиране на целева група
за кислородолечение при домашни условия.
Формиран
е екип, в който участват 3 лекари от клиниката по пулмология, рехабилитатор, кислороден
техник и 2 физика. Сключен е договори за наем на ползваното през първия етап
помещение с Медицинския университет - Плевен. По необходимата предварителна
информация е формирана първата целева група. Организирани са сеанси : три пъти
седмично по три часа кислородолечение, инхалаторно лечение с холинолитици и
дихателна рехабилитация. Подбрани са данните за контрол на здравния статус на
уточнените хора в групите за кислородолечение и контролната група.
В
ход са преговори за сключване на договори за снабдяване и поддръжка на
кислородното оборудване, необходимо за втората фаза на проекта.
2.
Създаване и приложение на информационно-експертен софтуер в ЦСМП с цел
повишаване ефективността на диагностиката и лечението на спешно болните
пациенти. Често затруднение в работата на екипите на Центъра за спешна помощ са
пациентите в тежко състояние, които не са в състояние сами да дадат сведение за
заболяването , което ги е довело , а оттук се стига до загуба на време до
изясняване на диагнозата, което пък забавя нужните лечебни мероприятия. В други
случаи поради здравно невежество пациентите и техните близки не съобщават на
лекаря важни подробности от здравният си статус. Създаването на База данни и
експертни модули спомагащи диагностиката и лечението на рискови пациенти, които
най-често попадат в ЦСП би спестило много време, скъпо струващи лабораторни и
инструментални изследвания,би повишило ефективността на терапията.
Така
възникна идеята, че ако спешният екип разполага с предварителна достоверна
информация за пациента и бърза справка и съвет от компютърния помощник, това би
улеснило диагностичното и терапевтично решаване на проблема.
При
първия етап на проекта ще се създаде базата данни, системата за управлението й
и апробация на реалното й използване На следващ етап ще се създадат експертни
модули, комуникиращи с информацията за отделния пациент от БД, спомагащи
вземането на диагностични и терапевтични решения.
При
направеното предварително проучване се оказа, че регистрираните в районните
поликлиники за 1995 година пациенти с тежка степен на хипертония 2172 души, с
ритъмни и проводни нарушения 382, епилептици 133,с бронхиална астма са общо 664
души, диабетици 3500 и т.н. Общо за град Плевен това са приблизително 7-8000
болни, които в определен момент поради остро усложнение на основното си
заболяване стават пациенти на ЦСМП.
Беше
формиран екип, в който участват лекари от СБМП и клиниката по пулмология, както
и асистенти от катедрата по Физика и биофизика.
При
първият етап се работи в две направления - събиране на предварителна
информация, необходима за попълване на таблиците в базата данни и реализиране
на първи вариант на БД. Уточнено е каква информация ще влиза за всяка
нозологична рискова група. На тази база до момента са събрани данни за: Астма -
>300, Диабет - >4000, Епилепсия
- >100, Хипертония - 1000, Инсулт -
200, Ритъмни и проводни нарушения -
>200. Информацията за съжаление е много непълна и това е голям проблем за
реалното и използуване при някои рискови групи.
Проведено
е инфологическо проучване за БД включващо: обзор на предметната област, определяне
и описание на обектите в БД, структурните връзки в БД, оптимизация. Създадена е
първата версия на БД и системата за управление на БД.
Подготвят
се обучаването на специалисти от СБМП за работа с информационната система и
нейното реално апробиране в практиката на центъра за спешна медицинска помощ.
ФормулЯр
Драги читатели,
Надяваме
се, че настоящото издание ви е било полезно. В случай, че някой от вашите
приятели се интересува от него, може да си го поръча, попълвайки следния
формуляр:
1.
Бих искал/а да получа пълния текст на следните статии:
а/
.......................................................................................................................................................................
б/
.......................................................................................................................................................................
в/
.......................................................................................................................................................................
2.
Коментари.
а/ препоръки
..........................................................................................................................................................................
..........................................................................................................................................................................
..........................................................................................................................................................................
..........................................................................................................................................................................
б/ в следващи броеве бих искал да се
публикуват материали по следните здравни проблеми:
..........................................................................................................................................................................
..........................................................................................................................................................................
в/ бих искал/а да публикувам в този бюлетин
следните материали:
/приложете ги отделно/
3. Адрес, на който искате да получите
посочените от Вас материали:
Трите Ви имена:
Улица:
Град/село
Област
Пощенски код:
Изпращайте
този формуляр и писма на следния адрес:
Висш медицински институт - Плевен
ул. “Св. Климент Охридски” N 1
Медицинска библиотека
5800 Плевен
Програма “Комуникации за по-добро здраве”
тел. 064/24765, E-mail: mailto:vmilibrpl@mbox.digsys.bg
Забележка:
За работещите по проекти в рамките на програмата "Решаване на проблеми за
по-добро здраве" резюметата от MEDLINE и евентуално пълните текстове на
статии се осигуряват безплатно по линия на програмата "Комуникации за
по-добро здраве".
Въпросник
За да Ви бъдем по-полезни по доставянето на здравна информация
в сферата на Вашите интереси, бихме искали да попълните следния въпросник:
Дата
на попълване:
А/
Лични данни
Вашето
име:
..........................................................................................................................................................................
Специалност:
..........................................................................................................................................................................
Къде
сте я придобили
..........................................................................................................................................................................
Кога
сте завършили
..........................................................................................................................................................................
Месторабота
в момента
Придобита
специалност /каква, кога/.
..........................................................................................................................................................................
Б/
Основни здравни проблеми в региона Ви
Кои здравни проблеми/заболявания/ са
най-сериозните и/или най често срещаните във Вашия район? Молим да бъдете
конкретни!
..........................................................................................................................................................................
..........................................................................................................................................................................
В/
Източници на информация
1.
Отбележете, като ги степенувате от 1 до 7, Вашите източници на здравна
информация:
Библиотека Колеги Монографии/учебници Списания
Практика Конференции
Други
/по възможност избройте/
..........................................................................................................................................................................
2.
Има ли пълен комплект от основните учебници по медицина във Вашата болница/на
работното Ви място? Да Не
/Подчертайте верния отговор/
Ако
отговорът е “Да”, повечето от заглавията след 1987 год. ли са публикувани?
Да Не
3.
Имате ли свободен достъп до тази литература?
Да Не
4.
Имате ли собствени медицински учебници?
Да Не
Ако
отговорът е “Да”, кои от тях са Ви най-полезни? Кога са издадени?
...................................................................................................................................................................…
…………………….………………………………………………………………………………………..
5.
Получават ли се редовно медицински списания на местоработата Ви?
Да Не
Ако
отговорът е “Да”, кои от тях са Ви най-полезни?
..........................................................................................................................................................................
.................………………………………………………………………………………………………….…
6.
Вие самите абонирани ли сте за някакво медицинско списание?
Да Не
Ако
отговорът е “Да”, избройте ги.
..........................................................................................................................................................................
..........................................................................................................................................................................
7.
Имате ли собствен каталог от заглавия по актуална медицинска информация?
Да Не
Ако
отговорът е “Да”, опишете го накратко / т.е. монографии, копия от статии,
изрезки от вестници, списания, лични бележки и др./
..........................................................................................................................................................................
..........................................................................................................................................................................
8.
Получавате ли лично и редовно безплатни материали от СЗО или други здравни
организации?
Да Не
Получават
ли се редовно такива материали във Вашата болница или работното Ви място?
Да Не
Ако
отговорът е “Да”, опишете ги накратко.
..........................................................................................................................................................................
..........................................................................................................................................................................
9.Осигурен
ли Ви е ли достъп до
а/
телефон Да Не
б/
факс Да Не
в/
електронна поща Да Не
г/
интернет Да Не
10.
Ползвате ли услугите на медицинска библиотека?
Да Не
11.
Кои услуги от библиотеката ползвате?
Заемате
книги Да Не
Заемате
книги по пощата Да Не
Посещавате
библиотеката Да Не
Поръчвате
библиографска справка Да Не
Поръчвате
копия от нужните
Ви
статии Да Не
12.
Кои от изброените по-горе услуги бихте ползвали най-често?
..........................................................................................................................................................................
..........................................................................................................................................................................
13.Посочете
кои от Вашите професионални занимания изискват периодична информация. Избройте
тези занимания накратко - грижи за пациента, обучение на студенти, научна
работа, следдипломна квалификация, други.
..........................................................................................................................................................................
..........................................................................................................................................................................
14.
Ще имате ли полза, ако Ви се предоставят копия от статии, третиращи
заболявания, които са сериозен проблем за Вашия район/регион?
Да Не
15
Ще имате ли полза, ако Ви се предоставят копия от статии от Ваши колеги,
третиращи заболявания, които са сериозен проблем за Вашия район/регион?
Да Не
Ако
отговорът е “Да”, по кои проблеми бихте искали да са те?
..........................................................................................................................................................................
..........................................................................................................................................................................
16.
Моля добавете своите коментари по въпроси, които считате за важни по отношение
на разпространението и достъпа до интересуваща Ви здравна информация, както и
своите предложения по осигуряването й.
..........................................................................................................................................................................
..........................................................................................................................................................................
..........................................................................................................................................................................
..........................................................................................................................................................................
Благодарим
Ви. Отговорите изпращайте на адрес:.
Висш медицински институт - Плевен
ул. “Св. Климент Охридски” N 1
Медицинска библиотека
5800 Плевен
Програма “Комуникации за по-добро здраве”
РедколегиЯ
Главен редактор: доц.д-р Кунчо Игнатов, к.м.н. - ректор на ВМИ - Плевен; Редакционен
съвет: проф. д-р Никола Мумджиев, д.м.н.; проф. д-р
Христо Браилски, д.м.н, доц. д-р Гена Грънчарова, к.м.н., доц. д-р
Григор Горчев, к.м.н., доц. д.р Мария Александрова, к.м.н, доц. д-р
Ташко Делийски, к.м.н., д-р Аспарух Георгиев, д-р Явор
Иванов, Отговорен секретар: Ст.пр. Янка Цветанова; Предпечатна
подготовка: ст.пр. Милко Цветанов, н.с. Валери
Русинов